

Exclusives
EXCLUSIVE: Prominent Trans Surgeon Admits In Unearthed Video That Complications Of Genital Surgery ‘Can Be Pretty Bad’
No featured image available
A prominent surgeon stated that the complications from vaginoplastic surgery that aims at removing male genitals and creating a vagina ‘can be pretty bad” and noted that there was “a growing number of programs throughout the world of gender affirmation, probably with a lack of training and not proper training,” according to the video of a presentation that the Daily Caller News Foundation obtained through a public records request.
“Complications can be pretty bad for vaginoplasty and the most-dreaded complication is to perforate the rectum while you are dissecting the vaginal cavity,” Dr. Alex Laungani, a Canadian surgeon, who has “expertise in trans surgical care,” said at an event sponsored by the World Professional Association for Transgender Health (WPATH).
“You are essentially dissecting the vaginal cavity between the prostate and the rectum and there’s literally no space there,” he said. “So, you have to create a new plain in a spot that doesn’t exist. So, you’re very close to the rectum and it’s very hard–it’s very easy to get in there. We don’t, I mean, the more you do it, the less risk you have, of course.”
WPATH is a medical organization that has published an influential clinical guidance on transgender health care called Standards of Care for the Health of Transgender and Gender Diverse People (SOC). Laungani’s presentation, entitled “Foundations in Surgery,” was part of an educational series recorded in September 2022 for licensed clinicians seeking WPATH certification in transgender health care. Laungani is a WPATH member,
The WPATH Standards of Care recommend that transgender surgeons be educated, trained and supervised on how to perform sex reassignment surgeries. However, Laungani said in his presentation that as the number of sex-reassignment programs had grown, it was likely some surgeons had not received adequate training.
“We’ve seen a growing number of programs throughout the world of gender affirmation, probably with a lack of training and not proper training, for now,” said Laungani. “And so, you know, better ca–any care was better, probably, than no care. So, it did allow individuals to have access to surgery. But it’s time just to make sure that we have the right training and that everybody has the same standard because the patients deserve it.
“And, so, we need to make sure that, you know, we’ll build these training programs, fellowships, and things,” he said. “And it’s really happening now. So, this is going to be something mandatory.”
“Well, you do great only what you do often, right,” Laungani said. “So, if you do a vaginoplasty every two years, I don’t think you could consider yourself proficient. You’re going to have more complications.
“You’re not going to follow up, you know, and you’re not going to be that interested that you actually go and hang out at these kinds of conferences and learn from your colleagues, because you’re not going to do it as much,” he said. “So, I think you need to dedicate a huge part of your practice to gender-affirming care if you are going to do it at all.”
WATCH:
In this WPATH presentation, Laungani gave an overview of vaginoplasty, a surgery that seeks to create a vagina by removing male genitalia, surgically creating a vaginal canal, and lining the canal with tissue which often comes from other parts of the body. Laungani discussed the details of a vaginoplasty procedure, saying: “So, you’ll use the skin of the penis to tack it down and invert it and start the beginning of lining of the canal. But you won’t have enough skin to line the entire canal–to some, there are some rare exceptions–so you’ll need some extra tissue there.”
Laungani said this tissue needed for the vaginal canal can be taken from the abdomen, scrotum, or colon. However, he warned that using colon tissue could increase the risk of complications.
“Or you could be using even a piece of colon,” he said. “So, to use colon vaginoplasty, um, usually that’s reserved for secondary deepening. We don’t do it as a primary intervention because it’s more morbid. You get to, you know, you have to cut bowel, you know it’s more, you may have, encounter, more complications,” said Laungani.
One article published in 2023 in the journal Plastic and Reconstructive Surgery stated: “Penile inversion vaginoplasty (PIV) is a common procedure for transfeminine patients, with the goal of creating a functional vaginal canal and clitoris and a natural-appearing vulva. Creation of the neovagina requires opening the prerectal space, most commonly from a perineal approach, and the reported rates of rectal perforation during this dissection range from 3% to 5%.”
A slide in the WPATH presentation listed possible complications of vaginoplasty, which include minor wound dehiscence, vaginal stenosis, recto-vaginal fistula, pelvic floor dysfunction, and clitoris necrosis.
During the presentation, Laungani noted the rate of wound dehiscence, a complication in which a surgical incision reopens, could be as high as 75%. “I think for the dehiscence you can expect as much as probably 75 percent,” he said.
In the recording, Laungani explained that within the first week after surgery, a vaginoplasty patient must begin regularly dilating the surgically created vagina, sometimes called a neovagina, to prevent closure. He described dilation as a sometimes painful, time-consuming process, saying patients have to dilate themselves up to four times a day.
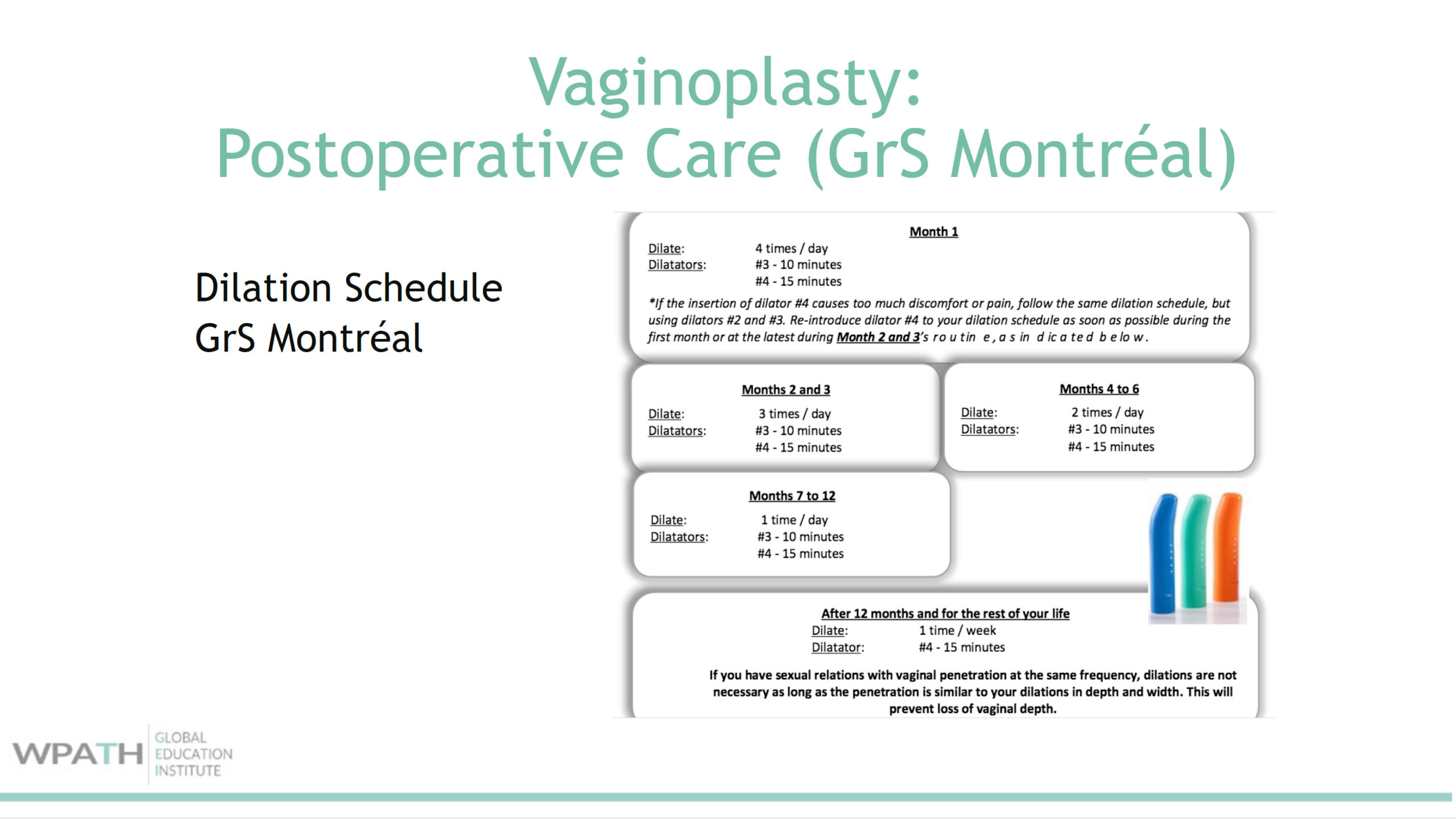
Screenshot from the WPATH Presentation Showing Dilation Schedule Following Vaginoplasty Surgery
“[A]s soon as we remove that vaginal stent, we start dilating because there will be a tendency from the body to want to contract and close that, considered as a wound sort of. So, you’ll have to fight that contraction and then dilate quite a bit at first. Which is, you know, what the patients call a full-time job for the first few months because it’s four times a day. It’s a lot,” said Laungani.
During a question-and-answer segment, Laungani was asked if there were any non-surgical interventions to redialate a neovagina that had not been dilated for approximately two years.
“That scar tissue is really rock hard. It’s like concrete. You can’t, once it’s settled, you won’t’ be able to just go, even with tiny dilators, and then increase the size of the dilators. It’s just not going to work. So, it has to be surgical,” responded Laungani.
Laungani was also asked about sexual function after vaginoplasty. “Can they orgasm still?” a person asked him.
“I wish we had more data on that,” Laungani said. “But the answer is: Yes, they can. For some individuals definitely do relate that–either by self-palpitation or through penetration or other sexual activities that they have around the clitoris.”
“The only thing we know is that there’s going to be more tendency to be able to orgasm if you were to, if you were able to orgasm before surgery. So, but you know, some, the patients who were not masturbating before surgery, then you would have potentially more issues to reach that orgasm after surgery,” Laungani said.
The Daily Caller News Foundation previously reported that Dr. Daniel Metzger, a WPATH certified pediatric endocrinologist, warned that if puberty blockers are started too early, boys may not develop the genital tissue needed to create a surgical vagina later in life.
“When you think about vaginoplasty, the creation of a vagina in an assigned male, you need tissue, genital tissue, to create that vagina,” said Metzger. “And if we are taking an 11-year-old boy, who does not have a lot of genital tissue and blocking puberty right there, we’re preventing the growth of the vagina for down the road.”
WPATH and Dr. Alex Laungani did not respond to a request for comment.
All content created by the Daily Caller News Foundation, an independent and nonpartisan newswire service, is available without charge to any legitimate news publisher that can provide a large audience. All republished articles must include our logo, our reporter’s byline and their DCNF affiliation. For any questions about our guidelines or partnering with us, please contact [email protected].